

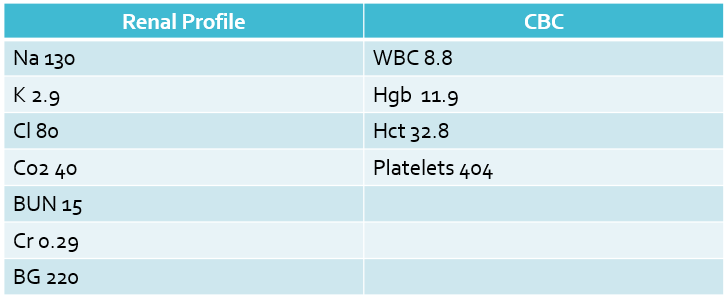
The patient has hyponatremia, with a hypochloremic, hypokalemic metabolic alkalosis.
Ultrasound!
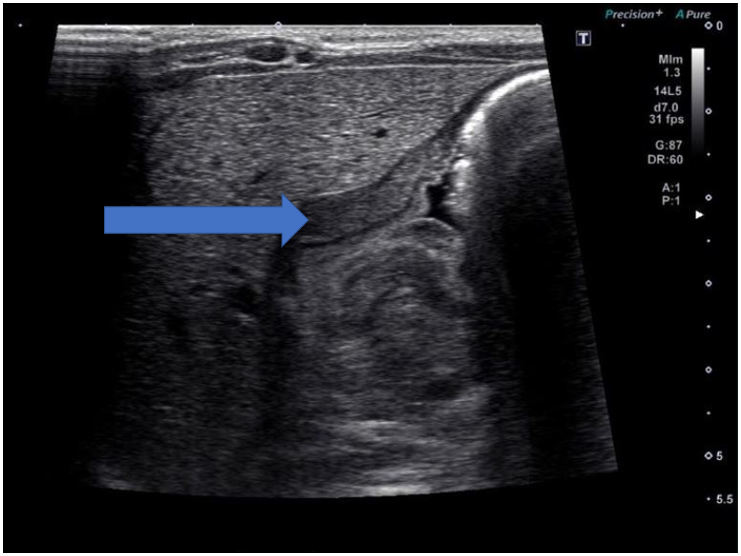
An ultrasound of the pylorus was obtained.
An easy way to remember if the pylorus is thickened or not is “Pi”lorus or 3.14. If the thickness of the pylorus is >3mm and >14mm in length, it is likely hypertrophic pyloric stenosis.
Hypertrophic Pyloric Stenosis
Classic presentation is a first born male at 3-6 weeks of age. The textbook history state there is “projectile” NBNB vomiting, through this history is difficult to obtain (many parents will describe any vomiting as “projectile”).
Classic lab findings are hypochloremic, hypokalemic metabolic acidosis, as seen in this case. Infants often are presenting earlier with increasing availability of ultrasound, so these lab abnormalities may not be seen. Ultrasound will show a thickened pylorus– remember your “Pi” mnemonic as described above.
Treatment is usually surgical correction.

Katie Edmunds is a current Pediatric Emergency Medicine Fellow interested in creating PEM 4 all those who are given the responsibility of treating the sickest babies wherever they may be.
