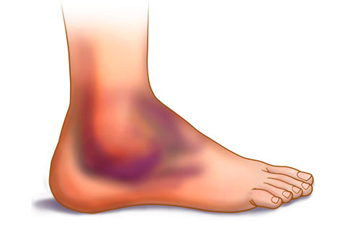
Here is what your patient's ankle looks like
How do you want to evaluate his ankle? What are the important questions to ask? Are there any rules you can use to help guide your evaluation and work up?

How do you want to evaluate his ankle? What are the important questions to ask? Are there any rules you can use to help guide your evaluation and work up?

