

The Case
You and your team are called to the resuscitation bay for a poorly responsive young child on a hot and muggy day. Low and behold his rectal temperature is 32 degrees Celsius and he is indeed obtunded. After managing the ABC’s, you take a step back and think about how you’re going to deal with the other problem.
Hypothermia
Managing the Cold
Staging
Hypothermia is defined as a core temperature below 35 degrees Celsius. It has various stages that are classified by the core temperature (Table 1).
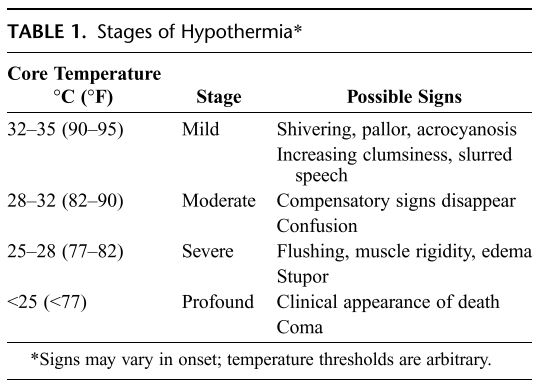
Table 1 shows the severity of hypothermia based on core temperature. Image comes from a study by Corneli et al.
The Differential
Hypothermia can be a primary concern in situations such as cold exposure in the winter months but also a secondary complication of a condition or derangement such as a submersion injury or sepsis, among other possibilities (Table 2) [1]. Delineating between the two can help direct the management plan and help address the secondary causes (i.e. identifying traumatic injuries).
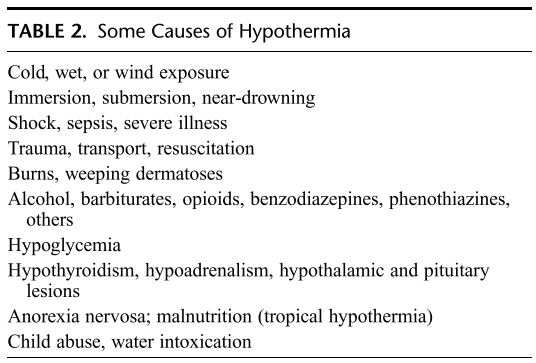
Table 2 showing different causes of hypothermia. Image comes from a study by Corneli et al.
Pathophysiology
The pathophysiology of hypothermia is complex and can affect vital signs, blood gas analysis, and impact medication effectiveness [1, 2]. There are also different complications that arise during care (such as rewarming shock, cardiac arrhythmias, and respiratory depression) which are independent of the cause of hypothermia [1, 2].
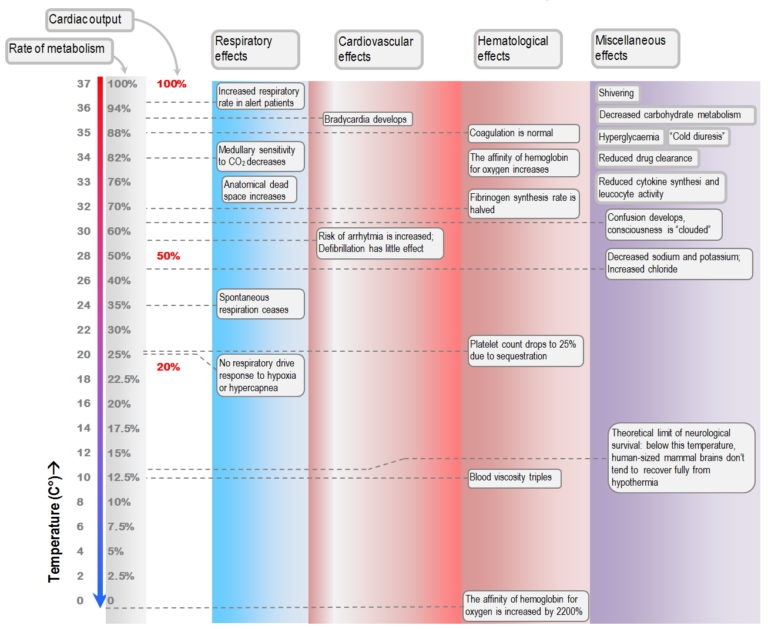
The image above shows different physiologic processes based on temperature. Image comes from Yarsev et al.
Treatment
There are numerous modalities for rewarming, which should be initiated promptly and in an appropriate manner for the clinical scenario. Modalities range from warm fluids, external rewarming, all the way to ECMO [2]. In situations where hypothermia is secondary to another cause, make sure to treat both concurrently.
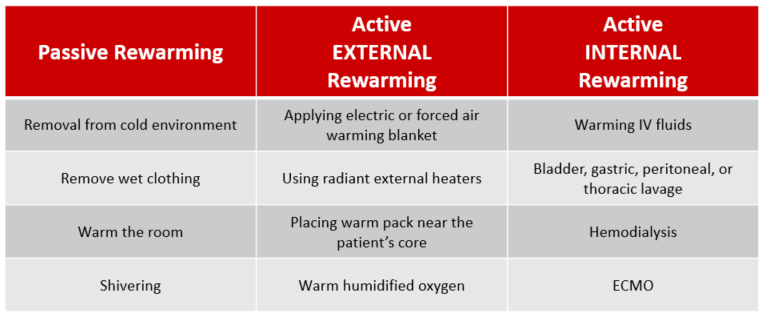
The image above shows different treatment modalities for hypothermia. Image adapted from Shah et al.
Case Resolution
Our patient was treated for sepsis and secondary hypothermia. Empiric broad spectrum antibiotics were started, and he was rewarmed with warm intravenous fluids, warm air via BiPap, and an external electric temperature control system. His temperature was 34 degrees Celsius after 2 hours and he was admitted to the ICU. His blood and urine cultures were both positive. During his treatment, he was never intubated, did not exhibit any cardiac arrhythmias or need pressors.
More great hypothermia reading
If you want to review more about hypothermia, in particular Accidental Hypothermia, check out this EMCrit Post and Podcast here. There is also great New England Journal of Medicine review article here.

1. Regardless of the cause of hypothermia (exposure vs sepsis) the pathophysiology is the same [1, 2].
2. Warming should happen concurrently in sepsis and core temperature may affect medication efficiency [1, 2].
3. Cardiac arrhythmias can happen at any point in hypothermia but the risk increases under 32 degrees Celsius; rewarming is the ultimate treatment for arrhythmias [1-4].
4. Hypothermia in sepsis carries an increased mortality risk, possibly indicating the severity of infection or contributing to the delayed recognition of sepsis (especially in adults) [5, 6]
- Corneli, H.M., Accidental hypothermia. The Journal of Pediatrics, 1992. 120(5): p. 671-679.
- Yartsev, A., Hypothermia. Hypothermia | Deranged Physiology. Derangedphysiology.com. Retrieved 14 August 2019, from https://derangedphysiology.com/main/required-reading/trauma-burns-and-drowning/Chapter%204.0.6/hypothermia, 2019.
- Rankin, A.C. and A.P. Rae, Cardiac arrhythmias during rewarming of patients with accidental hypothermia. British medical journal (Clinical research ed.), 1984. 289(6449): p. 874-877.
- Okada, M., The cardiac rhythm in accidental hypothermia. Journal of Electrocardiology, 1984. 17(2): p. 123-128.
- Young, P.J. and R. Bellomo, Fever in sepsis: is it cool to be hot? Crit Care, 2014. 18(1): p. 109.
- Kushimoto, S., et al., The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis. Crit Care, 2013. 17(6): p. R271.
- Scott Weingart. Podcast 66 – …Until they are warm and dead: Severe Accidental Hypothermia. EMCrit Blog. Published on February 7, 2012. Accessed on August 21st 2019. Available at [https://emcrit.org/emcrit/severe-accidental-hypothermia/ ]
- Brown, D. J., Brugger, H., Boyd, J., & Paal, P. (2012). Accidental hypothermia. New England Journal of Medicine, 367(20), 1930-1938.
- Shah, A.S, Madhok, M. management of Pediatric Hypothermia and Peripheral Cold Injuries in the Emergency Department. Pediatric Emergency Medicine Practice. 16(1) Jan 2019

